Afu’s ‘Bridge’ and the Doctor’s ‘Seal’: The Story Behind China’s Pioneering ‘AI + Doctor’ Collaborative Model
 06/17 2026
06/17 2026
 396
396

Yiyan Business Observer
Behind Ant Afu’s ‘AI + Doctor’ model, the Hippocratic Oath is being redefined for the digital age.
In a consultation room at the Fifth Affiliated Hospital of Sun Yat-sen University in Zhuhai, attending physician Li Jianjian faced a perplexing case: a young child presented with white patches on their leg that did not resemble vitiligo or common pityriasis alba. Dr. Li took a photo and uploaded it to the health AI application ‘Ant Afu,’ which promptly suggested a series of possibilities, including the rare condition ‘tuberous sclerosis’—a systemic disease affecting the nerves and skin, where early detection is critical. Guided by the AI’s insights, Dr. Li was able to intervene promptly, potentially averting a family crisis.

This scenario is not science fiction but the opening chapter of an ongoing healthcare revolution.
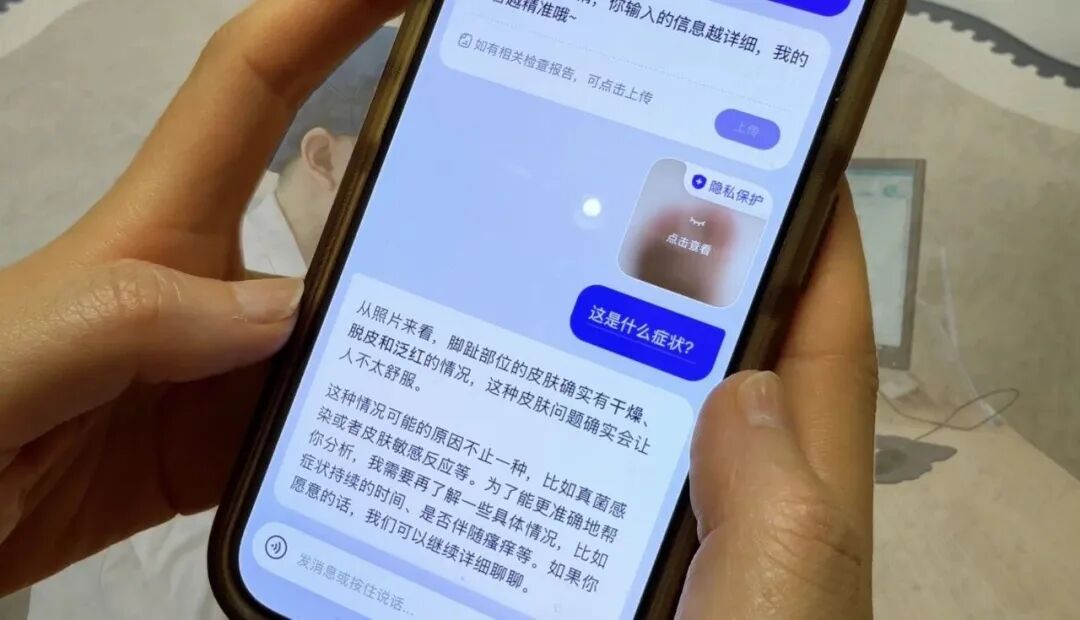
On June 15th, the health AI application ‘Ant Afu’ announced a significant upgrade to its ‘Skin Capture’ feature: the number of identifiable skin conditions expanded from 50 to over 100, covering 99% of common skin issues encountered in online consultations. However, what truly captured the industry’s attention was the simultaneous launch of the ‘Doctor Oversight’ function—after receiving AI responses, users can opt to have doctors from top-tier hospitals review the analysis and provide additional insights.
With a 15% user adoption rate, over 90% consistency between AI and doctor analyses, a doctor matching speed of approximately 5 seconds, and a full response time of 2 minutes, these metrics represent the achievements of China’s first AI application to implement the ‘AI Q&A + Doctor Oversight’ collaborative model.
In the past two years, as AI large models have rapidly advanced, the healthcare sector has grappled with an insurmountable ‘Theseus’s Ship’ dilemma: No matter how powerful AI becomes, who bears responsibility for patients’ lives?
Ant Afu’s breakthrough lies not in technological flair but in constructing a ‘bridge’ of human-machine collaboration that addresses the industry’s chronic issues and the implementation gap of AI. By introducing ‘Doctor Oversight,’ it anchors Theseus’s Ship with a human touch—ensuring that, regardless of AI’s capabilities, the ultimate responsibility rests with compassionate human professionals. Through this bridge, we witness the underlying logic and imaginative potential of the ‘AI + Doctor’ landscape being reshaped.
The Black Box of Trust and Healthcare’s Chronic Issues
To appreciate the transformative significance of ‘AI Q&A + Doctor Oversight,’ we must first examine the two major dilemmas it seeks to resolve.
The core pain point of the healthcare industry has remained fundamentally unchanged for years: the extreme scarcity and uneven distribution of high-quality medical resources. In top-tier hospitals, a chief dermatologist may see around 120 patients a day, averaging less than 5 minutes per patient. Doctors are overworked, and patients struggle to secure appointments. Meanwhile, a lack of trust in primary care leads patients to flock to top hospitals regardless of the severity of their condition, causing severe strain on medical resources.
AI is seen as a powerful tool to address these issues. However, from IBM Watson’s setbacks in oncology to the frequent inaccuracies of general-purpose large models in medical Q&A, pioneers have collided with a wall named ‘Trust and Responsibility.’ Medicine is not merely a science of information retrieval and comparison but a sacred trust involving lives. AI can provide suggestions based on probabilities but cannot bear the legal and ethical consequences of misdiagnosis. When patients see a cold, impersonal message like ‘possibly melanoma’ on a screen, it triggers immense panic and doubt. What if patients question the information provided by AI? Is there a more reasonable solution than rushing to the hospital? This is the ‘Theseus’s Ship’ dilemma of AI in healthcare: If all the planks of the ship are replaced by AI, is it still the same ship capable of bearing the weight of life?
Ant Afu’s answer is: Don’t replace everything. Let AI be the keel, and doctors the ballast. The ‘Doctor Oversight’ function essentially opens a window into AI’s black box, using personalized professional credibility to endorse the machine’s computational power.
Human in the Loop: ‘AI Quality Inspector’ and ‘Human-Machine Dual Safeguard’
Within the Afu App, a redefined medical ‘assembly line’ is in operation: AI initiates the consultation, outputs structured analysis and recommendations, users opt for ‘Doctor Oversight,’ the system matches an attending physician from a top-tier hospital within 5 seconds, the doctor reviews and confirms or supplements the consultation, closing the loop within 2 minutes.
This is not a simple superposition of ‘AI + Doctor’ but a profound reorganization of productivity: AI completes 90% of basic information collection and routine recommendation output, while doctors only need to perform 10% ‘confirmation’ and ‘supplementation’ at critical nodes. Zhu Jinjin, a dermatologist at Wuhan Union Hospital, summarizes it as: Doctors should not become ‘porters’ for AI but learn to be ‘quality inspectors’ for AI.
The role of the ‘quality inspector’ strikes at the heart of AI’s integration into healthcare. In traditional online consultations, doctors act as ‘full-stack engineers,’ handling everything from listening to the patient’s chief complaint to reviewing images and providing diagnoses—a time-consuming and highly repetitive process. In Afu’s model, AI handles the ‘initial screening’ and ‘standardized production.’ With the ability to identify over 100 skin conditions and cover 99% of common issues, AI has already filtered out and provided preliminary frameworks for most routine and mild cases.
Now, doctors are positioned later in the process. They are no longer frontline operators but the final ‘quality control checkpoint.’ The 15% user adoption rate during the testing phase precisely demonstrates that this is not redundant but addresses the rigid demand of patients who are skeptical of AI or have slightly more complex conditions. The over 90% consistency rate between AI and doctor analyses, in turn, proves the reliability of AI as a ‘primary productivity force.’
The doctors involved in Afu’s oversight process all come from top-tier hospitals across the country. Previously, the time of experts in top-tier hospitals was an extremely localized scarce resource; now, through AI platform distribution, a doctor can spare 5 minutes between two patients to provide ‘secondary confirmation’ to anxious patients in remote areas, transcending geographical barriers. The expertise of excellent doctors is amplified through the AI platform, achieving cross-regional equity. Director Gan Jiecheng of Shanghai Xinhua Hospital put it succinctly: For common minor issues, patients don’t necessarily need to visit a top-tier hospital; they can now receive a relatively reliable judgment at home. There might have been hesitation before, but with the oversight of experienced top-tier doctors, patients can generally feel at ease.

In Dr. Li Jianjian’s rare disease case, we see another layer of significance in this model: AI serves as an extra pair of eyes for doctors. A doctor’s experience is limited by individual exposure, while AI has access to a vast repository of authoritative medical knowledge. When AI includes rare diseases in its differential diagnosis, the doctor’s task shifts from ‘finding a needle in a haystack’ to ‘process of elimination,’ forming an increasingly smooth dual safeguard loop through human-machine collaboration.
This is precisely what futurist Kevin Kelly predicted as ‘Human in the Loop’: Humans remain an integral part of the loop, machines expand human capabilities, and humans set the boundaries for machines.
The Imaginative Potential of the ‘AI + Doctor’ Model
Why is dermatology the optimal breakthrough point for the ‘AI + Doctor’ model?
Dermatology relies heavily on visuals and is a typical ‘image-driven’ department, which happens to be the area where current multimodal large models excel. Additionally, skin issues are highly prevalent, mostly mild, and patients often require follow-up consultations, making it a natural source of traffic. However, this is just the beginning. The path proven by Afu opens up a vast blueprint for the entire ‘AI + Doctor’ landscape to evolve in depth.
From Single-Department Breakthrough to Full-Department Replication
Once the collaborative paradigm of ‘AI Initial Screening + Doctor Oversight’ is validated in dermatology, it will quickly extend to other departments highly reliant on visuals and data comparison, such as pathology, imaging, and ophthalmology. Even in the future, internal medicine consultations and general practice triage could adopt this model. AI becomes the ‘universal external brain’ for all doctors, while doctors serve as the ‘ultimate guarantors’ for all AI.
From ‘Occasionally Curing’ to ‘Often Comforting’ Service Elevation
In Dr. Lü’s consultation room at ‘Koukou Doctor’ in Shenzhen, we see a more humane commercial possibility. After AI takes over standardized knowledge output like ‘how to use medication, how to moisturize and protect from the sun,’ doctors’ time is freed up. Dr. Lü can now discuss recent stress and life troubles with patients because ‘skin diseases are also psychological; besides medication, we need to find the knot in the patient’s heart.’
The medical field has a famous Hippocratic Oath: ‘Occasionally cure, often help, always comfort.’ Previously, due to time constraints, doctors could barely achieve ‘curing’; now, empowered by AI, doctors can finally return to the essence of ‘helping and comforting.’ This provision of emotional value will be the core premium of future high-end commercial medical services.
Forcing the Digital Evolution of Medical Infrastructure
Xu Shuqiang, Dean of the China Hospital Development Institute, pointed out that this exploration will drive the integrated innovation of AI technology and professional medical services. When ‘Doctor Oversight’ becomes the norm, medical data will accumulate at an unprecedented rate through human-machine interaction. AI will evolve from a supportive ‘quality inspector’ to a ‘collaborator’ in clinical research, ultimately feeding back into new drug development, epidemic prediction, and public health decision-making, with a commercial extension in the trillions.
Conclusion: The Best Healthcare Is a Conspiracy Between Humans and Machines
Looking back years later, the significance of Ant Afu’s upgrade on June 15th for healthcare digitization may become clearer. It is not just a technological leap but a return to the essence of healthcare.
In the era of AI’s rapid advancement, people once feared that doctors would be replaced and that AI would spiral out of control. Afu provides the most straightforward answer: Let AI handle computation and breadth, and let humans handle trust and depth; AI covers the baseline for common diseases, and doctors guard the boundaries of rare diseases.

‘AI + Doctor’ is not a zero-sum game but a great conspiracy. When Director Liu Yi in Jinan easily schedules shifts on his phone, when Dr. Li Jianjian in Zhuhai illuminates dark corners with AI’s guidance, and when Dr. Lü in Shenzhen finally has time to listen to his patients’ inner struggles...we see the warmest side of technology shedding its cold exterior.
Kevin Kelly said that the ideal healthcare model is ‘AI + Doctor.’ Now, the blueprint has begun with Afu. When doctors and AI connect, they cast a wider net, catching not just anxious ordinary people but also humanity’s hope in combating disease and the unknown.
END
-
![]()
In-depth | Survival Transformation of 38 Million Freight Drivers: How Platformization Defines the Next Decade?
-
![]()
Why Have ‘Computing Power Rental’ Companies Emerged as the Biggest Winners in the AI Era Amid Soaring Chip Prices?
-
![]()
DeepSeek's Financing Details Revealed! How Liang Wenfeng Secured Control
-
![]()
Valued at 210 Billion Yuan, Generating 42 Billion Yuan in Annual Revenue, Xiaohongshu May Proceed with IPO
-
![]()
Three Straight Months of Growth in Heavy Truck Sales: Both New and Veteran Players Are on the Same Wavelength!
-
![]()
AI Rewrites the Logic of Going Global: Cross-border E-commerce Reaches a New Turning Point
-
![]()
DeepSeek Secures Over 50 Billion Yuan in Initial Funding Round: Tencent and CATL Among Investors
-
![]()
Trillionaire Musk