Where Should the Senior Citizens in County Towns Go?
 06/22 2026
06/22 2026
 475
475
By Guo Yihan
Original content from Evergreen Research Society
China has now entered a phase of profound aging. According to the <2026 National and China Silver Hair Economy Development Research Report>, the size of the elderly population in China continues to grow, while the number of new births continues to decline, resulting in a demographic shift characterized by an expanding elderly population and a shrinking younger one.
Amidst this aging trend, the urban-rural divide is widening further. By 2020, the proportion of the population aged 65 and above in rural areas had reached 17.72%, which is 6.96 percentage points higher than that in urban areas. Nearly a quarter of rural areas have transitioned into a super-aged society. Meanwhile, the declining birth rate has intensified the pressure on elderly care. In 2024, the number of newborns fell to 8.5 million, roughly half of the figure in 2000. With a continuously shrinking working-age population, the burden of elderly care is increasingly falling on county towns and rural areas.
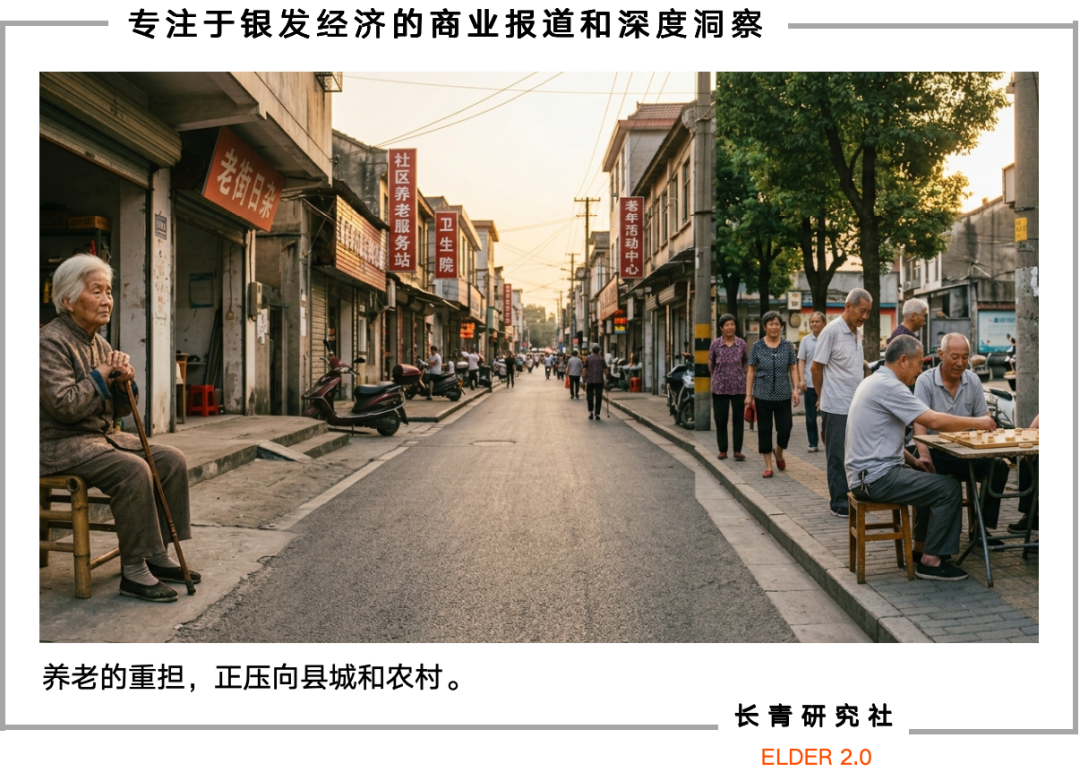
In this transformation of elderly care, the elderly in county towns and rural areas have emerged as one of the most easily overlooked groups in China's elderly care landscape. They remain deeply rooted in their rural backgrounds, unable to access the professional elderly care services available in cities, while facing the reality of their children moving to urban areas and the rapid weakening of family-based elderly care.
Elderly care has never been as simple as ensuring basic sustenance. The current aspiration for elderly care life can be further described as a transition to 'enjoying old age,' enabling the elderly to lead a more carefree and comfortable later life. However, the shift from 'elderly care' to 'enjoying old age' may still require step-by-step exploration in terms of grassroots policies and models.
Amidst various exploratory measures, where should the elderly in county towns, caught in the urban-rural divide, go?

The evolution of China's grassroots elderly care models is closely tied to social factors such as demographic structure and urban-rural development. Therefore, to understand the predicament of the elderly in county towns, we need to delve into the history of grassroots elderly care.
Initially, society did not face excessive pressure on elderly care, which was largely considered a 'private matter' for families.
From the founding of New China until before the reform and opening-up, the urban-rural divide kept rural society relatively isolated, and family-based elderly care was virtually the only model.
At that time, the rural population structure was relatively young. According to a paper by Yuan Xin, a professor at the School of Economics at Nankai University, titled 'The Changes, Dilemmas, and Improvements of the Chinese-Style Rural Elderly Care Model,' in 1964, the proportion of the population aged 65 and above in rural areas was only 3.66%, and the elderly dependency ratio was only 6.63, meaning that, on average, every 100 working-age individuals only needed to support 6.63 elderly individuals. Large multi-child families, rural filial piety ethics, and courtyard-style communal living formed the foundation of the most basic elderly care model, where children jointly shouldered the responsibility of supporting their parents, village norms reinforced the concept of 'respecting and honoring the elderly,' and land provided a basic livelihood for the elderly. Society relied solely on the 'five guarantees system' to support vulnerable elderly individuals with no one to depend on, without any concept of professional or socialized elderly care.
Later, the reform and opening-up marked a turning point. Accelerated urban-rural population mobility led a large number of young rural adults to migrate to cities, weakening the foundation of the family-based elderly care model. On the one hand, the family planning policy led to smaller family sizes, eliminating the pattern of multiple children sharing the pressure of elderly care; on the other hand, population outflow exacerbated empty-nesting, making it impossible for children to provide close care for the elderly, gradually diminishing the traditional function of family-based elderly care.
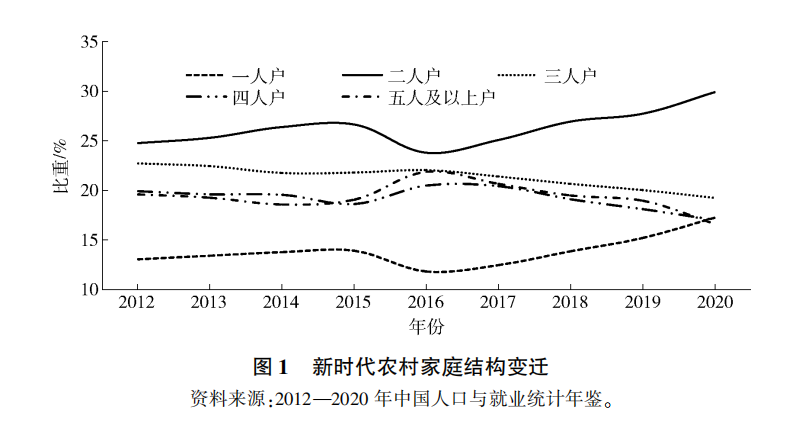
Miniaturization of rural family size
(Data source: 'The Changes, Dilemmas, and Improvements of the Chinese-Style Rural Elderly Care Model')
Although social elderly care began to emerge during this period, supply was far from meeting demand. Rural collective elderly care still only covered households under the five guarantees system, while private elderly care institutions were mainly family-run workshops with limited services and small scales, unable to meet the surging demand for elderly care. Therefore, grassroots elderly care faced a transitional period where families could not afford to support the elderly and society could not take over, leading to an imbalance in the supply-demand structure and highlighting the predicament of elderly care for the elderly in county towns and rural areas.
Currently, advanced age and empty-nesting have become the norm at the grassroots level, and families are clearly unable to independently shoulder the responsibility of elderly care. Grassroots elderly care has officially entered a new stage of collaboration among individuals, families, and society, forming a county-township-village three-tier system for implementation.
The county-level elderly care layer primarily undertakes functions such as centralized care for disabled elderly individuals, intelligent management of elderly care data, and personalized high-end elderly care services, integrating county-level medical resources to provide technical support for townships and villages; the township-level elderly care layer is responsible for centralized support for impoverished elderly individuals, bridging county-level resources and village-level needs; the village-level elderly care layer covers the vast majority of home-based elderly individuals, primarily providing welfare services such as home-based care, day care, community centers, and mutual support among lower-age elderly individuals.
Thus, it can be seen that grassroots elderly care has gradually formed a diversified pattern centered on home-based care, supported by communities, supplemented by institutions, and underpinned by medical care. However, the improvement of the model does not mean smooth implementation; there are still significant gaps between ideals and reality.

As mentioned earlier, the framework of grassroots elderly care has indeed become more comprehensive, shifting from family responsibility to tripartite collaboration. However, when it comes to county towns and rural areas, various mismatches and pain points make the path of elderly care challenging.
Both publicly built grassroots nursing homes and small workshop-style nursing homes pose significant inconveniences for the elderly.
In the grassroots context, one reason many elderly individuals refuse to enter institutional elderly care is the closed management, with gates tightly shut and restrictions on going out. 'Managed like a military operation, with the gates closed and no freedom to come and go, only allowed out twice a day for fresh air' is the current state of management in some publicly built institutional elderly care facilities.
This management approach contradicts the needs of grassroots elderly individuals who are 'attached to the land, their homes, and value interpersonal relationships.' Unlike urban elderly individuals, grassroots elderly individuals prefer an open lifestyle and socializing with acquaintances. This one-size-fits-all application of urban closed management has led to most institutions being 'affordable to build but not fully occupied.' Xia Zhuzhi, an associate professor at the School of Social Sciences at Wuhan University, has stated that the current construction of rural elderly care service projects mainly responds to top-down administrative tasks rather than truly addressing the common needs of rural elderly individuals.
Additionally, small workshop-style nursing homes, which low-income elderly individuals rely on, can provide more attentive services and emotional support but also face issues of safety compliance and operational costs.

This image shows a self-built elderly care institution in a rural area of a county town in North China
(Image source: The Paper People)
Chen Lu, a postdoctoral fellow at the School of Public Administration at Hubei University, found that most nursing homes converted from rural self-built houses lack land certificates and planning procedures, and their fire safety facilities cannot meet standards. Upgrading to meet standards would require higher costs, which small operators cannot afford. Some nursing homes have been shut down due to the inability to install fire sprinkler systems in the community, leaving low-income elderly individuals without their only elderly care option.
An even more challenging issue is the dual shortage of professional talent and services. Grassroots elderly care workers have low certification rates and high turnover. Township medical staff face the dilemmas of 'low salaries, tight quotas, and difficult promotions,' leading to continuous talent loss. Some grassroots elderly care workers lack professional training, and their services may be limited to 'laundry and cooking,' unable to meet the needs of disabled elderly individuals for rehabilitation and medical care.
Elderly individuals' reluctance to enter nursing homes stems from both concerns about social perception and trust issues.
Surveys in Zhongxian County show that elderly individuals worry about being seen as 'unfilial' by others if they enter institutions, while their children fear that institutional caregivers are unprofessional and that their parents will be mistreated. Moreover, frequent news reports of elderly individuals being abused in nursing homes or having their pensions scammed by institutional staff have exacerbated children's trust crisis in institutions. 'In a nursing home, with so many people, who will pay special attention to a particular elderly individual?' Some, worried about unprofessional caregivers, simply hire caregivers to come to their homes, 'so they can see the caregiver's every move and feel more at ease.'
Therefore, most elderly individuals choose home-based elderly care. However, this brings new problems, as the current family and individual caregiving capacities are far inferior to before.
Data shows that the average number of children for rural elderly individuals has dropped to 2.9, with more than 60% living alone or only with their spouses, resulting in a lack of intergenerational care from children; the average monthly income of rural elderly individuals is only 470 yuan, with pensions ranging from 100 to 300 yuan, providing meager and unstable income; nearly 70% of elderly individuals have only a primary school education or less, with insufficient health awareness, and their bodies have been worn down by years of farming, limiting their self-care abilities.
Currently, China has approximately 35 million disabled elderly individuals, accounting for 11.6% of the total elderly population, with a higher disability rate in rural areas than in cities. These elderly individuals who have lost self-care abilities may struggle to ensure even basic living needs, let alone self-care.
In fact, in response to the predicament of grassroots elderly care, the state has proposed the development of mutual support elderly care models.
'Mutual Support Community Centers' are relatively early and typical examples of rural mutual support elderly care. These centers gather the strength and elderly care resources of self-reliant elderly individuals aged 60 and above living alone, implementing self-help and mutual support in daily life and management. They represent a mutual support elderly care model that 'village collectives can afford, elderly individuals can afford to live in, and the government can support.'
This model has been affirmed by the Ministry of Civil Affairs and actively promoted nationwide, but the operation of mutual support community centers across the country has not been ideal.
The main reasons are the lack of funding, regulations, and service supply, making it difficult to sustain solely with village-level efforts. Moreover, relying on lower-age elderly individuals to care for higher-age elderly individuals, with generally low levels of compensation and payment, makes it difficult to obtain equal returns.
Therefore, this elderly care model sustained solely by villages is also difficult to sustain in the long run.

The future of the elderly in county towns cannot rely on simply copying urban models or depending solely on one party's efforts. It must be based on reality, following a localized, inclusive, and professional integrated path, ensuring that elderly care services meet the needs of the elderly and are suited to local resources to truly achieve implementation.
For grassroots elderly individuals, home-based elderly care may still be the first choice. The first step in solving the problem is to bring services to their doorstep.
Zhongxian County in Chongqing has established a comprehensive home-based elderly care network, following the standard of 'one center per township, one station per village community,' with 4 street elderly care service centers, 84 community elderly care service stations, and 25 township elderly care service centers built. Elderly individuals can access services such as meal assistance, bathing assistance, medical assistance, health check-ups, and entertainment just by stepping out their doors, solving the problem of home-based elderly individuals being 'unattended and inconvenienced.'
Rugao, a city in Jiangsu Province, stands as one of China’s pioneering county-level regions to embrace an aging society. It has developed an innovative 'chain-style' elderly care model that integrates 'institutions, communities, and homes.' This approach leverages long-term care insurance to subsidize professional services and categorizes care into two distinct types. 'Civil affairs' caregivers provide monthly 3-hour visits to serve low-income, five-guarantee elderly individuals (a category of vulnerable seniors supported by government subsidies), while 'medical insurance'-certified caregivers deliver weekly 1-hour professional care to disabled and demented elderly individuals, covering vital sign monitoring, incontinence care, and rehabilitation training.
Since 2019, Rugao has rolled out a 'long-term care insurance' system, extending coverage from employees enrolled in medical insurance to all individuals insured under the basic medical insurance program. Based on the disability level of home-based elderly individuals, the insurance fund subsidizes family care service fees, home-based services, and certain assistive device expenses.
For instance, severely disabled elderly individuals opting for home-based care receive 15 yuan per day in family care service fees, an annual 8,000 yuan allowance for assistive devices, and 58 complimentary home nursing services, including meal delivery, life self-care training, and vital sign monitoring. This enables them to access professional care without leaving their homes.
Zhongxian County, meanwhile, addresses concerns over unsafe elderly care institutions and eroding public trust.
In terms of safety, Zhongxian has invested over 30 million yuan to upgrade facilities, boosting the permit acquisition rate for food business operations and the equipment rate of fire safety facilities in elderly care institutions from 32% and 55% to 100%, respectively. Simultaneously, it has issued guidelines for constructing private elderly care institutions, offering on-site guidance during the preparation phase and advising against non-compliant institutions to eliminate safety risks at the source.
To rebuild trust, Zhongxian has integrated with a smart elderly care cloud platform, enabling real-time video surveillance of all 117 elderly care homes in the county. It has also promoted the 'Internet + bright kitchen and open stove + AI intelligent recognition' model, enhancing transparency in dietary safety for elderly individuals. Additionally, it has abandoned the rigid, military-style management commonly found in publicly funded institutions, opting instead for age-friendly renovations to create warmer, more welcoming nursing homes and gradually reshaping public perceptions.
To address medical access challenges, Zhongxian has not only established traditional Chinese medicine hospitals or clinics within elderly care homes but also facilitated partnerships. Thirty medical institutions in the county have signed medical-elderly care integration cooperation agreements with 114 elderly care institutions, forming consortia and opening green channels for referrals and admissions. Plans are underway to cultivate 2–3 comprehensive health and wellness institutions with dual medical and elderly care qualifications, creating 'integrated medical-elderly care' demonstration sites and forging a more professional, trustworthy care continuum from elderly care to medical services.
Moreover, by tapping into the grassroots acquaintance socializing—a hallmark of rural communities—local resources can be effectively mobilized to create alternative elderly care models.
Zeng Hong, a scholar at Wuhan University’s School of Political Science and Public Administration, suggests that grassroots elderly care can leverage village and community acquaintance networks. This involves mobilizing healthy, lower-age elderly individuals to provide care, companionship, and shopping services for higher-age and disabled seniors—a cost-effective and highly trustworthy approach that fosters greater comfort among the elderly. Simultaneously, local elites and elderly associations can be engaged, drawing on clan and village culture to encourage donations of funds and labor. Elderly associations can organize paired assistance and cultural-recreational activities to enrich seniors’ spiritual lives and rebuild rural mutual support networks. Additionally, vacant rural houses and land can be repurposed into elderly care stations and activity centers, enabling seniors to age gracefully in familiar surroundings.
Of course, the successful implementation of elderly care services also hinges on 'funding' and 'talent.'
Just as small counties cannot simply replicate urban elderly care models, the successes of Zhongxian and Rugao cannot be blindly copied elsewhere. Counties must consider their unique circumstances, including financial constraints and manpower availability, adopting tailored measures that align with local realities.

Where should the elderly in small counties go? To truly elevate 'elderly care' from merely meeting basic needs like food and clothing to enabling a fulfilling old age, relocating to high-end institutions or remaining passively at home may not be the optimal path.
Perhaps, for the elderly in small counties, true 'enjoyment of old age' means spending their later years with dignity, companionship, and security in familiar settings.
Ultimately, grassroots elderly care must transcend indicator-driven approaches, take root in local communities, and closely align with seniors’ needs. It requires dismantling resource barriers to ensure healthcare, services, and funding reach the grassroots level. Most importantly, it must reignite local warmth, bringing elderly care back to human connections and the essence of life itself.
Elderly care is the cornerstone of people’s livelihoods and a barometer of societal civilization. When home-based care includes in-home support, communities offer service stations, institutions provide safety nets, medical green channels are accessible during illness, and local companionship nurtures mental well-being, the elderly in small counties can truly transition from 'elderly care' to 'enjoyment of old age.'
And this, perhaps, is the path forward for grassroots elderly care and the original intent behind addressing population aging.
—FIN—
-
![]()
Wang Huiwen, Former Meituan Executive, Achieves 20-Fold ROI, Supports 24 AI Startups
-
![]()
Another AI Computing Power Unicorn Launches IPO! Founded by a Changjiang Scholar
-
![]()
OFILM Holdings Secures Zhongke Daojing, Marking a Significant Leap in the Optical Communication Industry!
-
What Will Be the Next Key Battleground for Large Models After AI Coding?
-
![]()
Leapmotor's Sales Soar, Yet Hidden Concerns Loom
-
![]()
China’s Action Camera Market Soars: 3.12 Million Units Sold in Six Months, DJI Secures 74% Dominance
-
![]()
Zhang Yiming: Strategic Retreat as a Path Forward
-
![]()
Exploring Charging for Some Features of QianWen App: Can It Follow the Path of Doubao?